We have now finished transferring the egg. The process, which took only 10 to 15 minutes, is over, but now the real waiting begins. And right now, you can't stop thinking about one thing: "What's going on inside me right now?"
Take a deep breath if that's you. You are not the only one. Right now, millions of women around the world are sitting and wondering, hoping, and wanting to know what happens in the first week after embryo transfer.
And to be honest? That curiosity is lovely. Even though you can't see or feel most of what's going on within your body right now, it's amazing. Your embryo is on a small, quiet journey. From breaking out of its shell to touching your uterine lining for the first time to slowly burrowing in and declaring, "I'm here."
This blog will be with you every step of the way on that adventure. We'll explain what your embryo is doing on each day, whether you had a Day 3 transfer or a Day 5 blastocyst transfer. This is based on the most recent research in reproductive science and clinical knowledge. No old myths. No hazy guesses. Just real biology that is backed up by facts and explained in a way that makes sense.
Because you have a right to know what's going on. And most importantly, you should feel peaceful while you wait. Let's get started.
Before We Begin - Understanding the Starting Point
Before we go into what's happening in your body each day, let's take a step back and make sure we're all on the same page about a few crucial things. There is a lot of uncertainty about the embryo transfer process, and we need to clear up one common misunderstanding straight away.
What Exactly Happens During Embryo Transfer?
Let's rewind just a little.
The embryo transfer surprisingly doesn't take long time. It usually only takes 5 to 15 minutes, and occasionally even less. Here's what happens: the doctor carefully puts the embryo into your uterus using a thin, soft catheter, which is a very narrow, flexible tube. Most clinics now use ultrasonography to guide this procedure. This means that your doctor can see exactly where the catheter is travelling in real-time, making sure that the embryo is implanted in the best area, which is usually in the upper-middle section of your uterus.
There is no need for surgery. So, no cut and no stitches. You're awake the whole time, and a lot of women say it feels like a Pap smear, which is a little unpleasant but not painful.
A lot of people become confused at this point, and it's really important to understand this:
The embryo is not "implanted" during the transfer.
This is a common misunderstanding about IVF. People use the word "implant" improperly, but in medicine, the transfer and implantation are two quite different things. The embryo is simply placed into the uterus during the transfer. It is like carefully placing a tiny seed on the ground. The seed is just there and hasn't taken root yet.
Your embryo will be floating freely in the uterine fluid when the catheter is taken out. This fluid is warm and full of nutrients - which your body has been getting ready for for weeks with the help of hormones and medications. At this moment, your body doesn't even know the embryo is there. There isn't a hormonal signal yet. No implantation. No hCG. A tiny group of cells is just resting there in the space your uterus has made for them.
And that's where the real journey begins.
Day 3 Transfer vs. Day 5 (Blastocyst) Transfer - Why It Matters
Before we go into the day-by-day calendar, there's one more thing you need to know that has a direct impact on when things happen in your body.
Not all embryos are moved at the same point in their growth. On Day 3 or Day 5 after fertilization, your clinic may have moved your embryo depending on your treatment plan. And the difference between the two is significant.
If you had a Day 3 transfer (cleavage-stage embryo):
Your embryo was moved when it had about 6 to 8 cells and was still in the very early stages of division. It hasn't made a blastocyst yet at this point. That implies it needs a few more days to grow after it's put in your uterus before it can even start the implantation process. Think of it as a traveler who got there a little early. They need to get settled in, get things in order, and be ready before they can really feel at home.
If you had a Day 5 transfer (blastocyst):
Your embryo was transferred as a blastocyst, a structure significantly more developed that has about 200 to 300 cells. At this point, the embryo has already divided into two main parts: one that will become the placenta is called the trophectoderm and the other which will become your baby is the inner cell mass. A blastocyst on Day 5 is almost ready to hatch and implant significantly sooner after transfer.
This is why the day-by-day timetable looks different for each type of transfer. In this blog, we'll cover both, so no matter where you are in this process, you'll know exactly what to do.
Here's a quick comparison to keep handy:
Day 3 vs. Day 5 Transfer Comparison
Factor
|
Day 3 Transfer (Cleavage Stage)
|
Day 5 Transfer (Blastocyst)
|
Cell count at transfer
|
6-8 cells
|
200-300 cells
|
Development stage
|
Early division
|
Differentiated (inner cell mass + trophectoderm)
|
Time to implantation
|
~4-5 days post-transfer
|
~1-3 days post-transfer
|
Needs further development in the uterus?
|
Yes - must become blastocyst first
|
No - ready to hatch
|
Implantation
|
Day 6-10 post-transfer
|
Day 3-7 post-transfer
|

The Role of the Endometrium
We talked about what your embryo is doing, however implantation is not a one-sided story. It takes two. Your embryo needs a location to land, and your uterine lining needs to be ready for it. Let's understand that side of the equation.
Day-by-Day - What Happens Inside Your Body After Embryo Transfer
Alright, this is the part you've been waiting for. A true, science-based, day-by-day breakdown of what your embryo is doing within your body after it has been transferred.
One thing I want you to remember throughout this whole section is this: It doesn't mean it's not happening just because you can't feel it.
Right now, your embryo is on a little, quiet, and powerful journey. And even though you can't see most of what's going on, it's nothing short of wonderful. Let's go through it together.
Day 1 After Transfer - The Embryo Settles In
If you had a Day 5 blastocyst transfer:
Your blastocyst is now floating gently in the uterine cavity, where it is suspended in a warm bath of uterine fluid that is full of nutrients, cytokines, and growth factors. Think of it as a perfectly prepared environment by your body (with the help of your medication) to welcome and nourish this embryo.
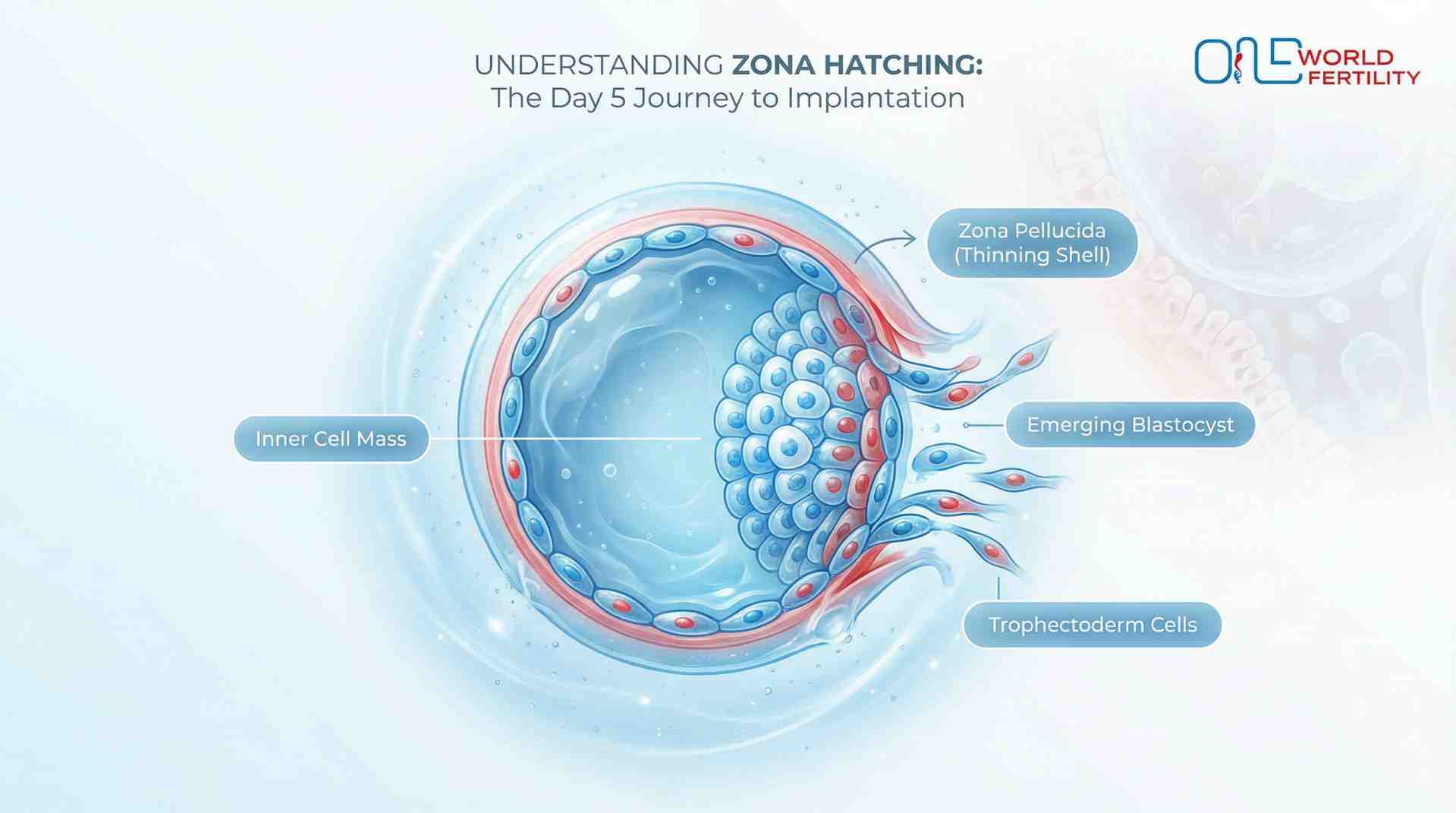
The blastocyst isn't just lying there on Day 1. It's starting to find its way about, slowly moving against your endometrial lining as if it's looking for the appropriate place to settle. At the same time, the zona pellucida, which is the thin, protective outer shell that has been around the embryo since it was fertilised, is starting to get thinner. It's getting ready for what's next.
If you had a Day 3 transfer:
Your embryo is still in development mode. It is still dividing, going from about 8 cells to the morula stage, which has about 16 or more cells. It is still completely surrounded by the zona pellucida and has not yet touched the wall of the uterus. This means it is on the right schedule, and there is no need to hurry.
What you might feel: To be honest? Nothing. And that's totally normal. Your body hasn't noticed the embryo yet. There is no hCG, no hormonal signal, and no implantation. It's quiet, and that is perfectly fine.
Day 2 After Transfer - Hatching Begins
If you had a Day 5 blastocyst transfer:
This is a crucial time: zona hatching. Your blastocyst is breaking free from the zona pellucida, which is its protective shell. Think of a baby chick breaking out of its egg, but on a microscopic scale.This must happen. Implantation can't happen without hatching. The trophectoderm, which is the outer layer of the embryo, needs to be able to touch your endometrial surface directly.
Your embryo got a head start here if your clinic did assisted hatching, which is when a small laser makes a hole in the zona pellucida before the transfer. Either way, at the end of Day 2, the trophectoderm cells that have been exposed are now touching the endometrial surface for the first time.
If you had a Day 3 transfer:
Your embryo is now in the morula stage, which means it contains 16 to 32 cells that are firmly packed together in a process called compaction. The cells are pushing against each other to make a solid ball. It's still growing and not ready to be implanted yet, but it's making great progress.
What you might feel: Most ladies don't feel anything at this phase. A few people say they feel very little bloating, but that's very definitely because of the progesterone drug, not the embryo. Don't think too much about it.
Day 3 After Transfer — Attachment Begins (Apposition & Adhesion)
If you had a Day 5 blastocyst transfer:
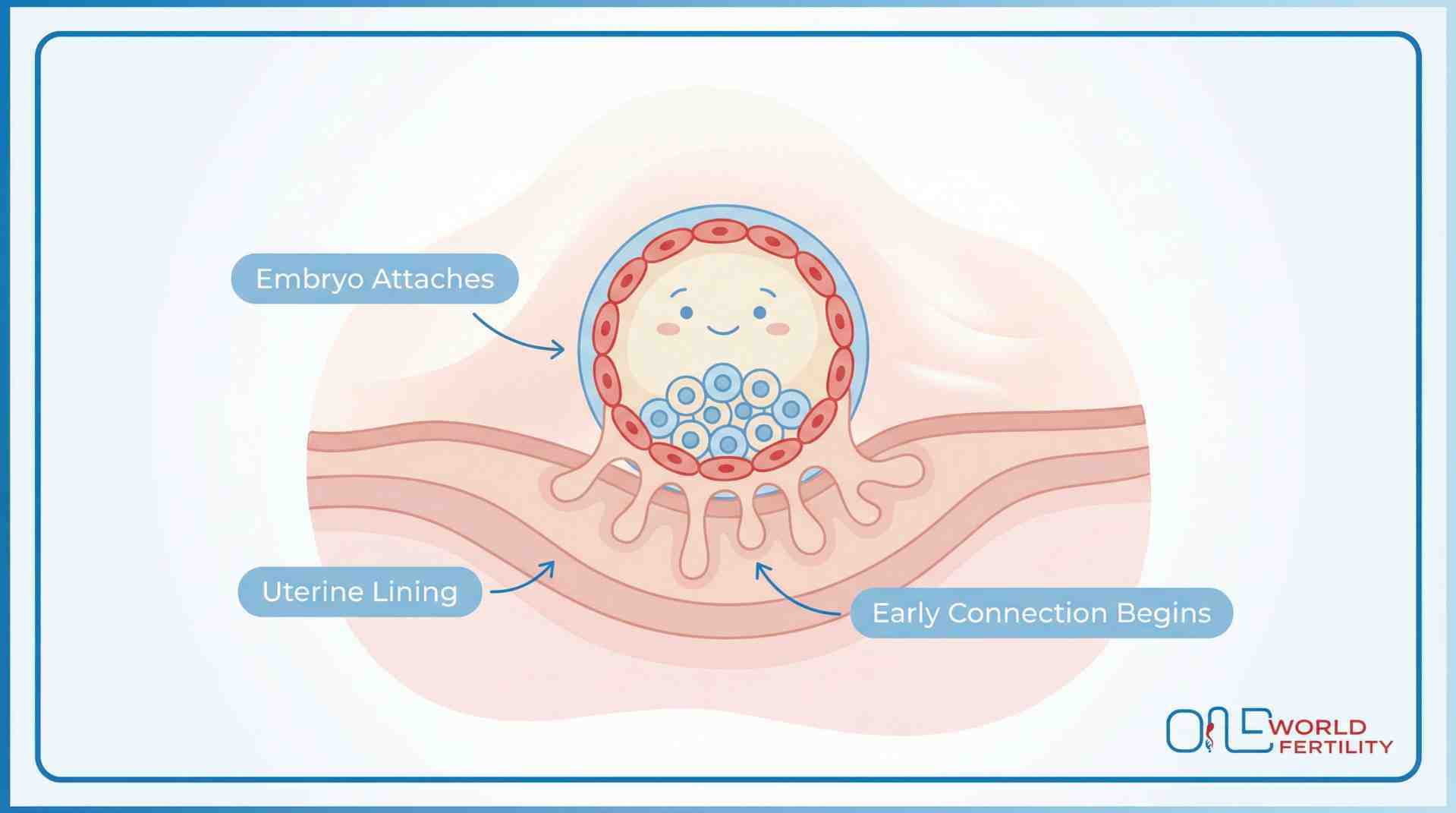
On this day, something amazing is going to happen. Your embryo starts to attach to the lining of your uterus and it is happening in two delicate phases.
Apposition is the first step. The blastocyst lightly touches the uterine surface. Picture the embryo softly "landing" on the lining, hovering just at the surface, testing the waters.
Then follows adhesion, which is where the magic happens at the molecular level. Your embryo and endometrium begin a chemical conversation. Integrins, selectins, and cytokines are molecules that scientists say make a "handshake" between the embryo and the uterus. Your endometrium is saying, "Yes, come in," and the embryo is saying, "Can I stay?"
The implantation window is short and it usually takes only 24 to 48 hours when the lining of your uterus is most open to receiving an embryo. During this period, small projections on the uterine surface called pinopodes assist to maintain the blastocyst in place.
If you had a Day 3 transfer:
Your embryo is changing from a morula to an early blastocyst. The blastocoel, a fluid-filled chamber, is beginning to form. And two main groups of cells are starting to separate: the inner cell mass, which will eventually become your baby, and the trophectoderm, which will become the placenta. It's still growing, but it's getting closer to being ready for implantation.
What you might feel: Some women say they feel slight cramps or light twinges around this time. Could this be the first clue that implantation is starting? Possibly. It might also be progesterone, digestion, or just your uterus getting used to things. You can't be sure, so pay attention to it but don't worry about it too much.
Day 4 After Transfer - Implantation Begins (Invasion)
If you had a Day 5 blastocyst transfer:
This is the big day. The real implantation starts.
The trophoblast cells, which are the outer layer of your blastocyst, start to break through the uterine lining. Yes, "invasion" is the real medical term. Your embryo is vigorously digging into the tissue of the uterine wall and trying to embed itself.
It may break small blood vessels in the endometrium as it digs. This is the biological reason for what some women call "implantation bleeding," which is light pink or brown spotting that some women detect around this time. Not everyone goes through it, and not going through it doesn't mean anything bad.
At this phase, the embryo is starting to make its first connections with your blood supply. These are the first threads of what will become the placenta.
If you had a Day 3 transfer:
The good news is that your embryo has been growing well in the uterus and is now a complete blastocyst. That protective layer on the outside? It's getting thinner, suggesting hatching is coming up soon. Your little one is just taking a slightly longer route than a Day 5 transfer, but it's still getting to the same destination. There are no delays, and nothing is wrong. It's working perfectly and at the proper speed.
What you might feel: This is when most people report implantation spotting, which is light pink or brown discharge that is usually quite little. Some women also have moderate cramps. Some people don't feel anything at all. These are all perfectly normal situations.
Day 5 After Transfer - Deeper Implantation & hCG Begins
If you had a Day 5 blastocyst transfer:
Implantation is deepening, and your embryo is now partially embedded in the endometrial lining, which means it is firmly settling into the wall of the uterus.
And this is the time when everything changes: the syncytiotrophoblast layer starts to form. This is a specialised, particular layer of cells that has one important job: to make hCG (human chorionic gonadotropin). The pregnancy hormone.
The production of hCG has officially begun. But remember, this is important; levels are still very low. We're talking about levels in the single digits. Too low for any home pregnancy test to find, and probably too low for a blood test as well. So please don't give in to the impulse to test.
The embryo is also starting to connect its early blood supply by making the structures that will become the placenta in the next few weeks.
If you had a Day 3 transfer:
Hatching has happened; your blastocyst has broken free from the zona pellucida. The embryo is starting to touch the endometrial surface for the first time. There is now molecular signalling going on between the embryo and your endometrium. Day 3 transfers have officially started the implantation process.
What you might feel: Some women feel more tired or have more sensitive breasts. But here's the truth: those symptoms are most likely caused by your progesterone medicine, not hCG, at this point. hCG levels are still too low for symptoms to show up.
Day 6 After Transfer - Implantation Completes
By Day 6, your embryo is firmly settled into the lining of the uterus, like a seed that has taken root. The lining has slowly closed around it. And now, for the first time, your body is getting the message. A small bit of hCG, the hormone that tells your body you're pregnant, is getting into your blood and gently saying, "
Something special is happening here." Your embryo is also making its initial link with you. It is forming early structures that will eventually become the placenta. And your body is reacting in the best way possible: by producing a soft, healthy space around the embryo and making sure your immune system protects it instead of attacking it.
This is all happening on its own. You don't have to do anything but trust the process.
If you had a Day 3 transfer:
Your embryo now starts to attach to the lining of the uterus and settle in softly, just like a Day 5 blastocyst did a few days ago. It's doing a great job of catching up. Some women may notice moderate cramps or light spotting around this time. If you do, don't worry. It could just be your embryo getting comfortable.
What you might feel: You might start to notice small changes, such as feeling a little sick, having a stronger sense of smell, or needing to pee more often. But the truth is that a lot of women still don't feel anything at this point. And that's just as normal as that. There is no connection between having symptoms on Day 6 and whether implantation was successful.
Day 7 After Transfer - hCG Rises and the Body Responds
If you had a Day 5 blastocyst transfer:
There are small but real levels of the hCG hormone in your blood now. Your body is getting the message: "There's a baby in here. Keep supporting it." Your ovary keeps making progesterone, the hormone that makes your lining thick, warm, and protective, which is exactly what your embryo needs right now.
We know what you're thinking: "Can I take the test now?" Most clinics will tell you to wait until Day 9 to 14 to have a blood test. And that's a good explanation. It can give false negative if testing too soon. This doesn't mean the test failed; it just means that the hormone levels aren't high enough yet to be detected early.
So, this is what we want you to remember from this moment: In just seven days, your embryo has broken free from its shell, landed on your lining, burrowed in, made its initial connection to your body, and begun sending signals that indicate "I'm here." Seven days. That's all it took for something absolutely amazing to start happening inside you.
If you had a Day 3 transfer:
Your embryo has found a place. It's settling into the lining and finding its place at home. The pregnancy hormone hCG has started to flow in your blood slowly. If you had a Day 3 transfer, your levels will be a little lower than someone who had a Day 5 transfer right now, but that's nothing to worry about. Your embryo just started the race a couple of days later, that's all. It's running the same race and crossing the same finish line, but at its own speed.
What you might feel: This is the time when a lot of women start to overthink every little thing. Feeling tired? Breasts a little sore? Bloated? Moody? Slightly nauseous?
Here's what we need you to hear:
You can't tell the difference between the signs of early pregnancy and the adverse effects of progesterone. They look alike. They feel the same. Doctors can't even tell them apart merely by looking at their symptoms. Your blood test is the only thing that will really tell you.
And what if you don't feel anything at all? That doesn't imply it didn't work. Many women who don't have any symptoms at this point go on to have healthy, strong pregnancies.
Please don't allow your symptoms (or absence of them) tell the story. The blood test will do that. Be nice to yourself until then. You've already gotten through the worst week.
Day-by-Day Summary - Day 5 Blastocyst Transfer
Day
|
What Your Embryo Is Doing
|
What You Might Feel
|
| 1 |
Floating gently in the uterus, finding its spot. The outer shell starts thinning.
|
Nothing - completely normal
|
| 2 |
Breaking out of its shell (hatching) and touching the uterine lining for the first time.
|
None, or mild bloating from medication
|
| 3 |
Landing softly on the lining and starting a chemical conversation with your uterus.
|
Mild cramping or twinges possible
|
| 4 |
Burrowing into the lining - this is when real implantation begins. Tiny blood vessels may be disturbed.
|
Light pink/brown spotting possible, mild cramping
|
| 5 |
Going deeper into the lining. The pregnancy hormone (hCG) starts being produced - but in very tiny amounts.
|
Tiredness, sore breasts - most likely from your medication
|
| 6 |
Fully settled inside the lining. hCG enters your bloodstream. Early placenta-building begins.
|
Subtle changes possible - or nothing at all
|
| 7 |
hCG is rising. Your body is getting the message that pregnancy has started.
|
Very early signs may show - or absolutely nothing. Both are normal.
|
Day-by-Day Summary - Day 3 Transfer
Day
|
What Your Embryo Is Doing
|
What You Might Feel
|
| 1 |
Still growing and dividing - building more cells inside the uterus.
|
Nothing
|
| 2 |
Cells are tightly pressed together, forming a compact ball.
|
Nothing
|
| 3 |
Starting to transform into a blastocyst - a hollow space is forming inside.
|
Nothing
|
| 4 |
Blastocyst is fully formed. The outer shell is thinning - hatching is close.
|
Nothing
|
| 5 |
Breaks out of its shell and touches the uterine lining for the first time.
|
Mild twinges possible
|
| 6 |
Starting to attach and gently push into the lining.
|
Light spotting or mild cramping possible
|
| 7 |
Settling in deeper. hCG production quietly begins.
|
Very subtle signs possible - or nothing at all
|
The Role of the Endometrium - Why Your Uterine Lining Matters
We've only talked about the embryo so far: its journey, its milestones, and its modest successes every day. But your uterine lining is another hero in this story that doesn't get enough attention. The embryo can only succeed if the lining is really ready to accept it, no matter how robust or healthy it is. So let's pay attention to your endometrium as it needs.
What Makes the Endometrium "Receptive"?
Your uterine lining isn't always "open for business." Your lining is actually in its most receptive state for a very short time, about 24 to 48 hours. This is what doctors call the "window of implantation." It's the one short time when everything in your uterus is ready to take in the embryo.
So what makes this window open? Three things work together:
- Thickness: The lining should be thick enough, and between 7 and 14 mm is best measured. Your clinic verifies this thickness before your transfer with an ultrasound.
- Hormonal preparation: Estrogen makes the lining thicker and richer by building it up during the first half of your cycle. Then progesterone comes in and transforms it into something soft, spongy, and nutrient-rich. This is why your progesterone prescription after the transfer is so important; it keeps the lining in this optimal condition.
- Your lining communicates with the embryo: During the window of implantation, the surface of your uterine lining makes unique molecules and tiny projections that reach out to the embryo and say, "You're welcome here." Come inside. It's like a tiny handshake that opens the door for your baby.
Even a perfectly healthy embryo won't implant if this window isn't open at the right time. That's how precise this process is.
What Happens to the Lining During Implantation?
Once the embryo starts settling in, your lining doesn't just sit there passively. It changes shape to shield and support the embryo. Here's what's going on:
- The cells in your lining change shape and swell, becoming specialised cells that provide nutrition. Imagine that your uterus is making a soft, warm, nutrient-rich cushion just for the embryo to rest on.
- Around the site of implantation, new blood vessels begin to grow. Your body is physically constructing a new way for blood to flow. This new path will eventually link your bloodstream to the growing placenta. This is how your baby will get food and oxygen during the whole pregnancy.
- Your immune system works together. This is the amazing part. Your body usually fights off anything that is "foreign." But here, it makes a smart and deliberate exception. Instead of attacking the embryo, specific immune cells surrounding the uterus assist it in settling in by keeping inflammation under control and promoting the formation of blood vessels.
Your body isn't fighting the embryo. It's welcoming it. And it knows just how to do it all by itself.
Can Endometrial Issues Affect Implantation?
Sometimes, even if the embryo is healthy, it doesn't implant. The lining can be the reason. Your doctor may check into these frequent problems:
- Thin lining (below 7 mm): It might not be thick enough to support implantation. If this keeps happening, your doctor can change your medication or look at other ways to help it grow.
- Polyps or fibroids: Little growths inside or near the uterus can make it hard for the embryo to find a healthy place to implant. Most of the time, they are found and treated before your transfer cycle starts.
- Silent infections: Chronic endometritis is a low-grade infection that doesn't always display symptoms but can make it harder for an embryo to implant. It's treatable with antibiotics. New research is also looking into the balance of bacteria in the uterus. Early results show that healthy bacteria in the lining may help IVF work, but more research is needed.
- Timing mismatch: The window of implantation opens a little earlier or later than predicted in certain women. Your doctor can use a test called ERA (Endometrial Receptivity Analysis) to find out exactly when your particular window opens. This is especially helpful for women who have had several failed transfers without a clear reason. However, it is not suggested for everyone.
Please know that if any of these things apply to you, it does not mean your body has failed. It just means that there is something definite that can be found, understood, and frequently fixed. Your doctor is looking at these things because they want to offer your embryo the best chance of success.

Hormones at Work - The Quiet Team Supporting Your Embryo
A group of hormones is working quietly behind the scenes to keep your embryo on track with all it is doing right now. You don't have to memorise them, but knowing the basics will help you feel more in control of what's going on.
Progesterone - The Most Important One Right Now
This week, progesterone is the hormone you need to know about. It's helping you in three big ways:
- Keeping the lining of your uterus thick, soft, and full of nutrients so the embryo may settle down safely
- Calming your uterus so that contractions don't happen, which could damage the embryo
- Keeping the lining intact - without progesterone, your lining would shed like a normal period.
The process of getting eggs for IVF can lower the amount of progesterone your body makes on its own. That's why your doctor has prescribed it, usually as vaginal suppositories, intramuscular injections, oral pills, or a combination.
You must not stop or skip your prescribed progesterone without your doctor's permission. This is the most important thing you have to do this week.
Estrogen - The Builder
Before your transfer, estrogen did its job by building and thickening your lining layer by layer. Now, it interacts with progesterone to keep that lining stable and whole. If your doctor has told you to take estrogen, keep taking it as instructed.
hCG - The Pregnancy Signal
This is the hormone that everyone has been waiting for. The hormone that pregnancy tests look for, hCG, starts to be made by your embryo after it implants. You should know this:
- hCG informs your body, "There's a pregnancy here - keep it going."
- It roughly doubles every 48 to 72 hours in the first few weeks of pregnancy.
- At Day 7 after the transfer, hCG levels are still too low for most tests to find.
- That's why your clinic tells you to wait until Day 9–14 for a blood test. They aren't trying to make you suffer; they want to give you a real answer.
Other Key Players
Your body also makes several additional substances, including LIF, cytokines, and VEGF, that assist the embryo in connecting, keep your immune system working, and make new blood vessels at the site of implantation. You don't have to memorise their names. Just know this, your body has an entire support team working behind the scenes right now, and they know exactly what to do.
Key Hormones and Their Roles in the First Week
Hormone
|
What It Does
|
Where It Comes From
|
Progesterone
|
Keeps the lining nourishing and stable, calms the uterus
|
the uterusYour ovary + prescribed medication
|
Estrogen
|
Built and thickens the lining before transfer
|
Your ovaries + medication (if prescribed)
|
hCG
|
The pregnancy signal - tells your body to keep going
|
Produced by the embryo after implantation
|
Others (LIF, VEGF, etc.)
|
Help embryo attach, build blood vessels, manage immune response
|
Your uterine lining and embryo
|
What Your Body Feels vs. What's Actually Happening
Let's talk about the big problem that affects practically every woman during the two-week wait: symptoms.
"I'm feeling crampy - does that mean implantation?" "Is it a good sign that my breasts hurt?" "I feel perfectly normal. Does that mean it didn't work?"
You're not the only one who has these thoughts. At this point in the IVF process, your thoughts can be your worst enemy. So let's be clear: no beating around the bush, no sugarcoating, and no lies.
The Hard Truth About Symptoms in the First Week
We know you don't want to hear this, but you need to hear it: The progesterone medicine is probably causing most of the symptoms you're having in the first week, not the embryo.
What Might Be Implantation vs. What's Definitely Medication
So can anything you feel actually be from implantation? Let's be honest about it:
- Light spotting: It could be implantation or progesterone. It's common in both cases.
- Mild cramps: The embryo could be settling in, or it could be a medication side effect, digestive discomfort, or simply your body adjusting. We can't tell what it is right now.
- Fatigue, bloating, sore breasts, and mood swings: These are all signs that your progesterone levels are at this stage.
- Not feeling anything at all: It is more common than you think. Many women without symptoms have healthy pregnancies.
The bottom line is? Pay attention to what you feel. Write it down if it helps you process. But don't give it any meaning. You can't tell if implantation worked by looking at the symptoms. Only a blood test can do that.
A healthier approach for this week:
- If you feel something, accept it. Don't suppress it.
- If writing helps you, do it. This is one of the good way to handle this kind of situation.
- Gently assure yourself by saying, "I'll let the blood test give me the answer."
- Spend less time on forums and posts that track your symptoms. Instead of that time, do something that makes you feel better, like going for a walk, listening to music, or talking to someone who makes you laugh.
- If your anxiety is too much, talk to your partner, a friend, or a therapist. You don't have to deal with this by yourself.

What Can Support or Hinder Implantation During This Week
Now let's be realistic: you can't control implantation, but you can make sure your embryo has the highest chance of success.
Things That Support Implantation
- Don't forget to take your progesterone, estrogen, or pregnancy vitamins on time, every time. This is the most important thing you have to do.
- Eat well. Leafy veggies, eggs, nuts, avocado, whole grains, and salmon are all good examples of foods that can help reduce inflammation. Think of feeding instead of limiting.
- Another important thing is to drink 8 to 10 glasses of water every day.
- Get enough sleep, like 7 to 8 hours. While you sleep, your body makes the most important hormones.
- It is good to take a light walk. It helps the uterus get more blood. You don't have to stay in bed, and you shouldn't.
- When you're stressed, your cortisol levels go up, which can make it harder for blood to reach your uterus. Anything that calms you down, like a walk, some music, deep breathing, or a talk with someone you trust, is good for you.
What to Avoid
- Don't stop or change your medicines without your doctor's permission, especially progesterone.
- Do not do hard workouts or heavy pulling, as these can cause your uterus to contract.
- Follow WHO and ASRM advice and daily caffeine intake limit to less than 200 mg, which is about one normal coffee.
- No alcohol. Even small amounts can alter the environment in which the embryo will grow.
- No smoking, even around other people who smoke. It narrows blood vessels, so less blood reaches the uterus.
- You have to avoid hot baths, saunas, and steam rooms; a high body temperature can make pregnancy more difficult.
- Painkillers like ibuprofen should not be taken unless your doctor tells you to. They might get in the way of the normal process your body needs to implant. Most people think paracetamol is safe, but you should always check with your doctor first.
Myths You Can Stop Worrying About
An awful lot of myth is floating around the internet. Let's clear up a few things based on facts.
- "I need to be on bed rest after transfer" - Incorrect. Several tests have shown that staying in bed doesn't help. In fact, it might make your chances a little worse. It's always a good thing to move slowly.
- "What if I sneeze or cough and the embryo falls out?" - It can't. Your embryo is very small and is held in place by fluid in your uterus. It won't come off no matter how hard you sneeze, laugh, or walk.
- This idea that "I should eat pineapple core for implantation" is not backed up by scientific proof, and it's not a fertility treatment.
- "I have to lie flat after the transfer." which is also not true. It's safe to stand and move around.
Final Thoughts
There's something amazing going on in your body right now that you can't even feel. In just seven days, your embryo has hatched, landed, burrowed in, and started sending its very first signals. So, it doesn't matter if you have all of the signs or nothing at all; the process will still work. It just needs some time.
You've done what you could. As you move into the second week, your hCG levels will rise, your first blood test will be coming up soon, and your body will start to react more clearly. Remember that each day is bringing you one step closer to finding out the answer.
That's why One World Fertility is here for you whenever you need help, support, or just someone who gets it. Every step.
Frequently Asked Questions
Most clinics schedule a blood test (beta hCG) between Day 9 and 14 after transfer. Home pregnancy tests can sometimes detect hCG earlier, but they're far less reliable and can show false negatives - simply because hCG levels are still too low. Testing too early and seeing a negative result can cause unnecessary heartbreak. Trust your clinic's timeline - it's designed to give you the most accurate answer possible.
Focus on balanced, nourishing meals - not a strict diet. Include anti-inflammatory foods like leafy greens, eggs, avocado, nuts, salmon, and whole grains. Stay well hydrated with 8–10 glasses of water daily. Limit caffeine to under 200mg (roughly one coffee). Avoid alcohol completely, raw or undercooked fish, and heavily processed foods. You don't need to eat perfectly - just eat with care.
During IVF, the egg retrieval process can reduce your body's natural progesterone production. But progesterone is essential - it keeps your uterine lining thick, nourishing, and stable so the embryo can implant safely. It also calms the uterus by preventing contractions. Without supplemental progesterone, the lining could break down. That's why it's the one medication you should never stop without your doctor's guidance.
Absolutely not. This is one of the most common myths in IVF. Your embryo is microscopic - far too small to be affected by physical movements like sneezing, coughing, laughing, or even walking. It's held securely within the uterine fluid. No normal daily activity can dislodge it. So please - laugh freely, sneeze without fear, and go about your day with confidence.
For a Day 5 blastocyst transfer, hCG production begins around Day 5–6 after transfer - but in extremely small amounts. By Day 7, it's entering the bloodstream. However, levels are usually too low for accurate testing until Day 9–14. For Day 3 transfers, hCG production starts a couple of days later. That's why your clinic asks you to wait - testing too early can give a misleading result.
A Day 3 embryo is transferred at the cleavage stage - about 6–8 cells - and still needs a couple more days of development inside the uterus before it can begin implanting. A Day 5 embryo (blastocyst) is transferred with around 200–300 cells, already fully developed and ready to hatch and implant sooner. Both can lead to healthy pregnancies - the timeline just differs slightly.
No. Multiple clinical studies and current medical guidelines (2024–2025) confirm that bed rest after embryo transfer offers no benefit - and may actually slightly reduce your chances. Your embryo is microscopic and held securely by uterine fluid. Walking, gentle movement, and resuming normal daily activities is not only safe but encouraged by most fertility clinics worldwide.
Yes, light spotting after embryo transfer is common and usually nothing to worry about. It can be caused by implantation, where the embryo disturbs tiny blood vessels as it burrows into the lining. It can also be caused by vaginal progesterone irritation. The spotting is typically light pink or brown and very minimal. However, if you experience heavy bleeding or soaking through a pad, contact your doctor immediately.
Most women feel nothing during implantation - and that's completely normal. It's a microscopic event happening at a cellular level. Some women report mild cramping or light spotting around Day 4–6 after a Day 5 transfer, but these same symptoms can also come from progesterone medication. There's no reliable way to tell the difference. Feeling nothing does not mean it didn't work.
After embryo transfer, your embryo floats freely in the uterus and begins a step-by-step process. For a Day 5 blastocyst, it hatches from its shell within 1–2 days, makes contact with your uterine lining by Day 3, and starts burrowing in by Day 4. By Day 6–7, it's fully embedded and producing hCG - the pregnancy hormone. For Day 3 transfers, this timeline shifts about 2–3 days later.